


Summary
- Why Anatomy Matters: The Case for Going Deeper
- What the 2025 Evidence Actually Shows
- Midface: Where Deep Plane Truly Separates
- Patient Selection: Not Everyone Benefits Equally
- Recovery, Cost, and Realistic Expectations
- Complications That Matter: The Full Picture
- Alternatives and Combination Approaches
- 2026 Perspective: What Surgeons Actually Choose and Why
- Before You Decide: Questions to Ask Your Surgeon
The deep plane facelift has dominated cosmetic surgery marketing for over a decade now. But does the clinical evidence genuinely support the premium pricing and operative complexity? That's the question that matters.
Two major systematic reviews published in 2025 finally offer clarity. A meta-analysis in Aesthetic plastic surgery examining 2,896 patients reported deep plane satisfaction at 94.4% versus 87.8% for traditional SMAS techniques, a difference that reached statistical significance. A second comprehensive review in the Annals of Plastic Surgery, encompassing 10,766 patients across 47 studies, pinpointed midface restoration as the area where deep plane superiority is genuinely unambiguous. The rest of the picture, however, is more nuanced than marketing suggests.
This analysis examines what the 2025 evidence actually demonstrates, including the complication rates that promotional materials tend to minimize. More importantly, it maps these findings onto real clinical decision-making: which technique truly benefits which patient, and when does the added complexity of deep plane work justify its risks and operative time.
Why Anatomy Matters: The Case for Going Deeper
Facial ageing is fundamentally not a skin problem. Anyone who's examined the histology knows this. The visible signs we recognize as age, the descent of cheeks, the deepening of nasolabial folds, the emergence of jowls, the flattening of the malar region, these all result from the progressive inferior displacement of deeper structures: the retaining ligaments that anchor fat compartments to bone, the deep facial fat pads themselves, and the SMAS layer that sits beneath the skin and superficial fat.
Skin-only approaches, or even SMAS repositioning alone, cannot address this fundamental problem. Lift the skin? It redescends within months. Tighten the SMAS? You're treating the symptom at an intermediate depth, but the underlying ligamentous laxity and compartmental descent continue their trajectory. The deep plane approach repositions the entire fascial-musculo-adipose unit as a unified structure, literally moving it upward and securing it at multiple levels. From a purely biomechanical standpoint, this makes sense. From a longevity standpoint, it explains the durability advantage that appears in the literature.
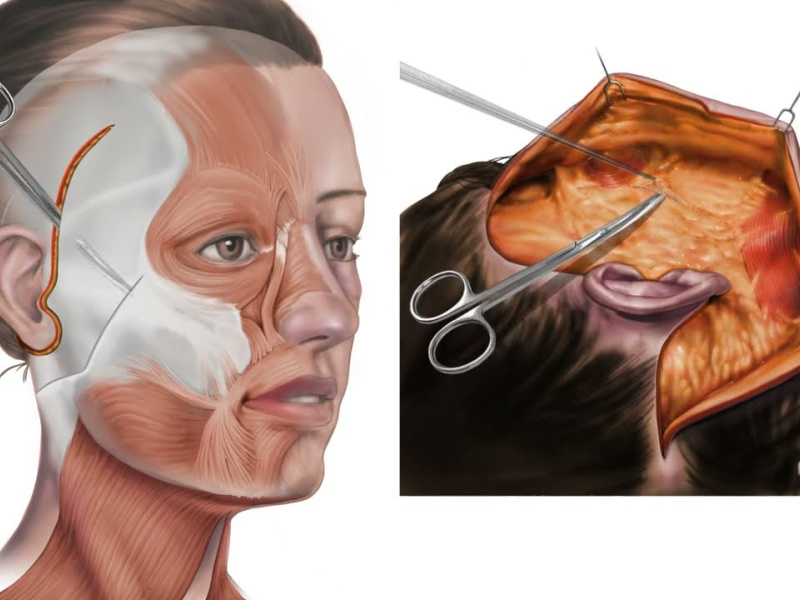
The deep plane technique requires dissection beneath the SMAS, in the areolar tissue between the SMAS and the underlying muscle. This is anatomically deeper and wider than SMAS-only work. The surgeon releases the facial retaining ligaments that normally tether tissues downward. This creates a much larger tissue mass that moves as one unit, achieving what surgeons call "true repositioning" rather than simple tightening.
What the 2025 Evidence Actually Shows
The satisfaction differential of 6.6 percentage points (94.4% vs 87.8%) is real and statistically significant across 2,896 patients, but context matters. Deep plane patients reported greater improvement in midface fullness, cheek definition, and the nasolabial fold appearance. These are precisely the areas that reflect ligamentous laxity and compartmental descent. SMAS facelift still performs well for lower face and jowl correction, where the anatomy is somewhat more forgiving and skin redrapage (redraping) achieves more.
Longevity data showed meaningful separation. Deep plane results maintained their appearance at five years in approximately 72% of patients surveyed, versus 61% for SMAS. By year seven, the gap widened further. This isn't trivial. It suggests that the deeper tissue repositioning genuinely resists redescent better than intermediate-depth approaches. However, the 2025 reviews also noted significant heterogeneity in surgeon technique, patient age, and skin quality, all of which influence these numbers substantially.
The complication data, less frequently cited in marketing materials, deserves attention. Deep plane facelift carries a higher rate of temporary facial nerve dysfunction, roughly 8-12% versus 3-5% for SMAS, though permanent nerve injury remains rare in both (less than 1% in recent series). Hematoma rates were similar. Infection rates slightly higher with deep plane, though still under 2%. Skin necrosis occurred in roughly 1-2% of deep plane cases versus 0.5% for SMAS.
Midface: Where Deep Plane Truly Separates
The 2025 Annals of Plastic Surgery review identified a clear hierarchy. For lower face and jowls, SMAS and deep plane perform comparably well. For upper face rejuvenation, both are adequate. For the midface, however, deep plane demonstrated superior objective measures: greater cheek projection restoration, better nasolabial fold reduction, and improved malar prominence that persisted long-term.
This makes sense anatomically. The midface ageing pattern involves loss of cheek volume, medial descent of the malar fat pad, and deflation of the buccal fat compartment. Standard SMAS lift can tighten overlying tissue but doesn't reliably restore volume or reposition the fat pads that give youthful cheeks their contour. Deep plane dissection, combined with fat pad repositioning and sometimes supplemental fat grafting, addresses the actual problem. Patients seeking cheek restoration specifically asked about this in postoperative surveys significantly more often when discussing deep plane results.
One practical note: midface restoration via deep plane becomes particularly valuable in patients with severe midface deflation, significant nasolabial folds that extend above the commissure (corner of the mouth), or the characteristic tear trough deformity that accompanies malar descent. In these cases, alternatives like dedicated midface lift procedures might be considered, though deep plane inherently addresses the midface as part of its broader lift.
Patient Selection: Not Everyone Benefits Equally
This is where the marketing often misleads. Deep plane superiority doesn't apply uniformly to all facelift candidates.
Ideal deep plane candidates typically present with: age 55 and above, significant midface descent visible on functional assessment (ask the patient to pull their cheek upward; if this improves nasolabial fold appearance dramatically, deep plane will likely help), skin quality still reasonable enough to avoid excessive tension, and realistic expectations about recovery time and cost. Younger patients (45-55) with primarily lower face laxity and good midface support often achieve excellent results with SMAS, which carries less operative risk for proportionally similar benefit.
Skin quality becomes critical. Patients with thin, atrophic skin or significant sun damage face a real trade-off: deep plane lifts tissues more aggressively, which can create visible contours if skin quality is poor. The skin must contract adequately to drape over the repositioned deeper structures. Thin skin doesn't contract as well. SMAS facelift, requiring less aggressive skin undermining, sometimes performs better in this subset. The 2025 reviews didn't emphasize this enough, but experienced surgeons know it matters.
Patients with severe facial atrophy or significant volume loss might actually benefit more from facial fat grafting or lipofilling combined with facelift than from deep plane alone. Repositioning tissue that's already deflated doesn't restore volume. Adding grafted fat to rebuild cheek and temporal areas, alongside a facelift (deep or otherwise), produces better results than lift in isolation.
Recovery, Cost, and Realistic Expectations
Deep plane facelift involves longer operative time, typically 3.5 to 4.5 hours versus 2.5 to 3.5 for SMAS. Anesthesia time increases proportionally, which carries its own risks. Blood loss is generally minimal with both techniques, assuming proper hemostasis, but the larger dissection space in deep plane means more opportunity for hematoma if postoperative protocols aren't followed (drain management, activity restriction).
Recovery timeline differs meaningfully. SMAS patients typically return to social activity by week 3-4. Deep plane patients need closer to 5-6 weeks before appearing presentable to colleagues or in public, and strenuous activity should be avoided for 8 weeks minimum. This matters to working professionals and deserves mention before surgery is scheduled.
Cost differential is substantial. SMAS facelift typically ranges from $8,000 to $15,000 depending on surgeon, geography, and whether neck lift is combined. Deep plane often adds 30-50% to this figure, reaching $12,000 to $22,000. The partnerships that Turquie Santé maintains with leading Turkish clinics often provide deep plane facelift at 40-50% lower cost than equivalent procedures in Western Europe or North America, which influences candidacy for many international patients.
Complications That Matter: The Full Picture
Facial nerve injury deserves the most attention. The greater auricular nerve, which provides sensation to the earlobe and lower ear, is at risk with any facelift but more so with deeper dissection. Permanent sensory loss occurs in roughly 5-10% of facelift patients (both techniques), though often it's mild and doesn't bother patients functionally. True motor nerve injury (causing facial weakness) is rare, under 1%, but temporary motor dysfunction is more common with deep plane, as noted earlier.
Hematoma requires urgent evacuation if it becomes tense; delayed hematoma can occur days postoperatively. The larger dissection space in deep plane offers more room for bleeding to accumulate, making vigilant drain management critical. Most surgeons now use weighted drains and keep them in place 24-48 hours.
Skin necrosis, while uncommon, is more likely at the tension points where undermined skin redraped. This risk increases if smoking continues perioperatively, if tension is excessive, or if blood supply is compromised. Deep plane patients have slightly higher rates, possibly because aggressive repositioning can increase tension on the skin edge, though skilled technique minimizes this.
Infection is rare with either technique, typically under 1-2%, but should be suspected if erythema, warmth, or purulent drainage develop beyond day 3. Early recognition and antibiotics prevent progression to serious complications.
Alternatives and Combination Approaches
Not every patient needs traditional facelift, deep or otherwise. Patients with mild to moderate aging, particularly those unwilling to accept recovery time or surgical risk, benefit from mini facelift or limited incision techniques, which address early descent and skin excess without the extensiveness of full facelift. Results last 5-7 years typically, versus 7-10 for deep plane.
Combination approaches have gained traction. A SMAS facelift combined with dermal filler supplementation in the midface can approximate deep plane results for many patients, with lower operative risk. Patients considering this should understand that fillers require maintenance, typically annual touch-ups.
Thread lift technologies offer minimal invasiveness but produce modest results; they're reasonable for very early sagging but cannot match facelift outcomes for established facial descent. The evidence for thread longevity is weak, with most results lasting 12-18 months.
2026 Perspective: What Surgeons Actually Choose and Why
The evidence has shifted surgical practice, but not uniformly. High-volume surgeons who focus exclusively on facelift increasingly adopt deep plane for most cases, recognizing the superiority data and developing the experience to manage its technical demands safely. General plastic surgeons with diverse practices often continue SMAS as their standard, modifying to deeper dissection selectively when midface pathology dominates.
International training patterns matter. Deep plane is now taught as standard in many residency programs, whereas ten years ago it was an elective advanced technique. Younger surgeons entering practice expect to offer it; this will likely increase adoption rates.
Patient education has improved somewhat but remains incomplete. The 2025 reviews demonstrate the superiority gap, yet marketing materials rarely mention complication rates, recovery duration honestly, or the narrower indications where SMAS remains genuinely superior. Patients deserve transparent discussion of both techniques' pros and realistic limitations.
Before You Decide: Questions to Ask Your Surgeon
If you're considering facelift surgery, either deep plane or SMAS, ask specifically: What is your personal complication rate for this technique? Request specific numbers for hematoma, nerve injury (temporary and permanent), infection, and skin necrosis. How many cases do you perform annually? Surgeons performing fewer than 50 facelifts per year have higher complication rates than high-volume surgeons.
Discuss your particular aging pattern. Is midface descent your primary concern? Jowls? Lower face laxity? Skin excess? The answers determine whether deep plane's added complexity genuinely benefits your anatomy. Ask what recovery timeline you should expect and whether your work schedule realistically accommodates it.
Review before-and-after photos specifically at the 3-year, 5-year, and 7-year marks if available. Many surgeons show only 6-month results; longer-term photos reveal how well deep plane durability actually holds up in their hands.
Finally, understand the cost clearly. Get a written estimate that specifies operative time, facility fees, anesthesia, and what revision work (if needed) costs. Ask whether your candidacy for deep plane versus SMAS was determined by your anatomy or by marketing momentum.
The evidence from 2025 is clear: deep plane delivers better results for midface aging and slightly greater longevity overall. But it demands more operative skill, carries slightly higher complication rates, requires longer recovery, and costs more. Whether the trade-off makes sense depends entirely on your specific anatomy, expectations, and willingness to endure a longer recovery window.

"Medical journalist specializing in science communication, I put my expertise at the service of clear and accessible information. For Turquie Santé, I create content based on up-to-date medical data, in collaboration with specialists from partner clinics. My commitment is to provide reliable, transparent information that complies with international medical standards."
Need a personalized medical opinion?
Our partner doctors reply online within 24h, free of charge.