A rapid heart rate, sudden pallor, and difficulty breathing following trauma, these are warning signs that should never be ignored. Internal bleeding can be life-threatening even when there is no visible wound.
What is internal bleeding?
Internal bleeding, medically termed hemorrhage, occurs when blood escapes from the vascular system (arteries, veins, or capillaries) and accumulates inside the body's cavities or tissues, with no external exit point. Unlike a surface cut, this type of bleeding is invisible to the eye, making it particularly dangerous: the patient may appear stable while losing dangerous amounts of blood internally.
The most common sites of internal hemorrhage include the abdominal cavity (hemoperitoneum), the chest (hemothorax), the brain (intracranial hemorrhage), the retroperitoneal space, and the tissues surrounding major bone fractures. According to the World Health Organization, traumatic hemorrhage accounts for approximately 1.9 million deaths per year globally, making it one of the leading causes of preventable death from trauma.
Clinical perspective: In emergency medicine, internal bleeding is classified by severity: Class I (loss of up to 15% of blood volume, minimal symptoms), Class II (15–30%, anxiety, tachycardia), Class III (30–40%, marked hypotension, confusion), and Class IV (over 40%, immediately life-threatening). This classification, known as the ATLS hemorrhagic shock grading, guides the urgency and type of intervention.
Symptoms of internal bleeding
Symptoms vary considerably depending on the location of the hemorrhage, the rate of blood loss, and the patient's baseline health. In many cases, especially following high-speed trauma or with slow-onset bleeds, the patient may feel fine initially, which is precisely what makes this condition so deceptive.
The most commonly reported signs include:
- Cold, clammy skin
- Rapid, weak pulse (tachycardia)
- Drop in blood pressure (hypotension)
- Dizziness or vertigo
- Fainting or loss of consciousness
- Rapid breathing (tachypnea)
- Pallor of the skin and mucous membranes
- Intense, unexplained thirst
- Nausea or vomiting
- Severe abdominal or chest pain
- Anxiety and restlessness
- Progressive confusion or agitation
Location-specific symptoms
The symptoms of internal bleeding also depend heavily on where the bleed is occurring. Abdominal hemorrhage may cause rigidity of the abdominal wall and referred pain to the shoulder (Kehr's sign, typically indicating splenic rupture). Intracranial bleeding typically presents with sudden severe headache, vomiting, unequal pupils, or neurological deficits. Gastrointestinal bleeding may manifest as dark, tarry stools (melena) or blood in vomit (hematemesis). Bleeding into a joint space (hemarthrosis) causes rapid swelling and intense pain.
It is important to note that in cases of hemorrhagic shock, the patient may be surprisingly calm or even confused, not necessarily distressed. This blunted presentation should not be misread as reassurance.
Main causes of internal bleeding
Internal hemorrhage can originate from a wide spectrum of causes. While traumatic events are the most well-known triggers, non-traumatic causes are equally important to understand.
Trauma-related causes
These causes are directly linked to physical injuries that damage internal organs or blood vessels.
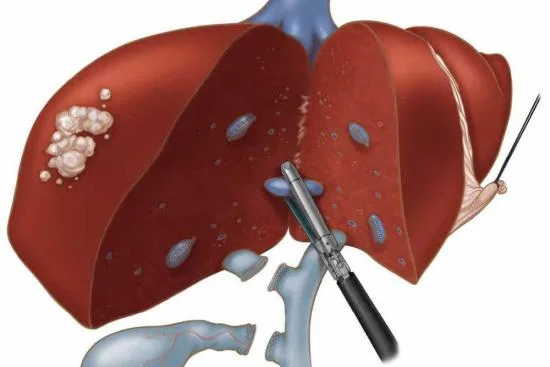
- Road traffic accidents: High-impact collisions frequently cause liver or splenic lacerations, pulmonary contusion, and aortic injury, all capable of producing rapid, life-threatening blood loss.
- Pelvic and femoral fractures: These are among the most hemorrhage-prone injuries. A fractured pelvis alone can result in the loss of 1.5 to 3 liters of blood into the retroperitoneal space. Femoral fractures can account for 1 to 2 liters of hidden blood loss.
- Abdominal, thoracic, and renal trauma: Blunt or penetrating injuries to these regions can rupture solid organs or major vessels.
Medical and obstetric causes
These causes occur without external trauma and are often related to underlying diseases or pregnancy complications.
- Ectopic pregnancy rupture: When a fertilized egg implants in the fallopian tube rather than the uterus, the tube may rupture as the pregnancy grows, triggering sudden, severe internal bleeding into the pelvis. This is a true obstetric emergency, most commonly occurring between weeks 6 and 10 of pregnancy.
- Obstetric hemorrhage: Uterine rupture (particularly during labor in women with a prior cesarean scar) or placental retention after delivery can cause massive postpartum bleeding.
- Gastrointestinal hemorrhage: Peptic ulcers, esophageal varices (linked to liver cirrhosis), Crohn's disease, diverticular disease, and colorectal cancer are among the leading causes of internal GI bleeding. In severe cases, angiography (CT angioscanner) is used to identify the bleeding vessel.
- Aortic aneurysm rupture: A ruptured abdominal aortic aneurysm is one of the most rapidly fatal forms of internal bleeding, with mortality exceeding 80% without immediate surgical intervention.
- Intracranial hemorrhage: This may result from hypertensive crisis, anticoagulant therapy, arteriovenous malformations, or hemorrhagic stroke (cerebrovascular accident).
- Postoperative complications: Internal bleeding can occur after surgery if a vessel was not adequately ligated or if a suture fails, particularly in the days following abdominal, cardiac, or orthopedic procedures.
High-risk groups
These groups have a significantly higher risk of developing internal bleeding due to specific medical or physiological factors.
- Patients on anticoagulants: Warfarin, heparin, or DOACs (rivaroxaban, apixaban) significantly impair clotting and increase hemorrhagic risk.
- Elderly patients: Vascular fragility, polypharmacy (especially NSAIDs + anticoagulants), and increased fall risk.
- Patients with hypervascular tumors: Certain cancers (hepatocellular carcinoma, renal cell carcinoma) can bleed spontaneously.
- Patients with coagulation disorders: Hemophilia or von Willebrand disease substantially increase bleeding risk, even from minor trauma.
- Pregnant women: At risk for ectopic rupture (early pregnancy) or obstetric hemorrhage (delivery).
- Chronic alcohol users: Associated with liver cirrhosis and esophageal varices, a dangerous source of GI bleeding.
What to do before the ambulance arrives: first aid steps
If you suspect someone near you is experiencing internal bleeding, following an accident, a fall, or a sudden collapse, the following steps can make a critical difference while waiting for emergency services:
- Call emergency services immediately: Describe the circumstances clearly, mechanism of injury, symptoms observed, patient's level of consciousness.
- Position the patient appropriately: If conscious and breathing normally, lay the patient flat on their back and elevate both legs 20–30 cm (the Trendelenburg-like position) to improve venous return to vital organs. If the patient is unconscious but breathing, place them in the lateral recovery position. If breathing is labored, allow a semi-sitting position.
- Keep the patient still and warm:Unnecessary movement can worsen a hemorrhage. Cover the patient with a blanket to prevent hypothermia, which worsens coagulopathy (the "lethal triad" in trauma: hypothermia, acidosis, coagulopathy).
- Do not give food, water, or any medication: In particular, never administer aspirin or ibuprofen, these inhibit platelet aggregation and can significantly worsen bleeding. Even water by mouth is contraindicated if surgery may be needed.
- Stay with the patient and monitor their condition: Speak to them calmly and reassuringly. Monitor breathing, skin color, and level of consciousness. Report any changes to emergency services when they arrive.
Important: Do not attempt to "wait and see" if internal bleeding is suspected. Unlike external wounds, you cannot apply pressure or see the bleeding. The only effective treatment is hospital-based. Time to treatment is the single most important factor in survival.
Hospital diagnosis and treatment of internal bleeding
Once the patient arrives at the emergency department, a structured protocol is followed, typically aligned with the ATLS (Advanced Trauma Life Support) guidelines used in hospitals internationally.
Diagnostic workup
- FAST ultrasound (Focused Assessment with Sonography in Trauma): A bedside ultrasound performed within the first minutes of arrival to detect free fluid (blood) in the pericardial, thoracic, and abdominal cavities. Fast, non-invasive, and highly effective for ruling in hemoperitoneum or hemothorax.
- CT scan with contrast (CT angiography): The gold standard for identifying the site and extent of internal bleeding. Particularly essential for abdominal, pelvic, and thoracic injuries. In GI bleeding, CT angioscanner can pinpoint the bleeding vessel when endoscopy is non-diagnostic.
- Blood tests: Complete blood count (CBC), hemoglobin and hematocrit levels, coagulation profile (PT, aPTT, INR), blood typing and crossmatch, lactate levels (as a marker of tissue hypoperfusion), and arterial blood gas analysis.
- Chest and pelvic X-rays: Rapidly obtained in trauma bay to screen for pneumothorax, hemothorax, and pelvic ring fractures.
Emergency treatment options
- Damage control resuscitation: Large-bore IV access, isotonic fluid resuscitation, and early administration of packed red blood cells, fresh frozen plasma, and platelets in a 1:1:1 ratio (balanced resuscitation), aimed at restoring circulating volume while minimizing dilutional coagulopathy.
- Tranexamic acid (TXA): An antifibrinolytic agent proven in clinical trials (CRASH-2) to reduce mortality when administered within 3 hours of traumatic hemorrhage. Now widely used in trauma protocols.
- Interventional radiology (embolization): For certain types of bleeding, particularly pelvic, hepatic, or splenic, transcatheter arterial embolization (TAE) allows selective blocking of the bleeding vessel without open surgery.
- Emergency surgery: Required in cases of uncontrolled hemorrhage, solid organ lacerations, bowel injury, aortic rupture, or ruptured ectopic pregnancy. "Damage control surgery" focuses on bleeding arrest and contamination control, with definitive repair deferred to a second procedure once the patient is stabilized.
- Endoscopic hemostasis: For upper or lower GI bleeding, endoscopy (gastroscopy or colonoscopy) can be both diagnostic and therapeutic, using clips, injections of epinephrine, or thermal coagulation to stop the bleeding.
- Correction of coagulopathy: In patients on anticoagulants or with clotting disorders, reversal agents (vitamin K, prothrombin complex concentrates, idarucizumab for dabigatran) are administered alongside surgical treatment.
Clinical outcome context: Prognosis for internal bleeding is highly variable. Isolated splenic trauma in a stable young patient may be managed non-operatively with a survival rate exceeding 95%. By contrast, a ruptured abdominal aortic aneurysm carries a mortality rate exceeding 80% without emergency surgery. Early recognition and rapid escalation remain the strongest predictors of survival.

"Medical journalist specializing in science communication, I put my expertise at the service of clear and accessible information. For Turquie Santé, I create content based on up-to-date medical data, in collaboration with specialists from partner clinics. My commitment is to provide reliable, transparent information that complies with international medical standards."
Need a personalized medical opinion?
Our partner doctors reply online within 24h, free of charge.