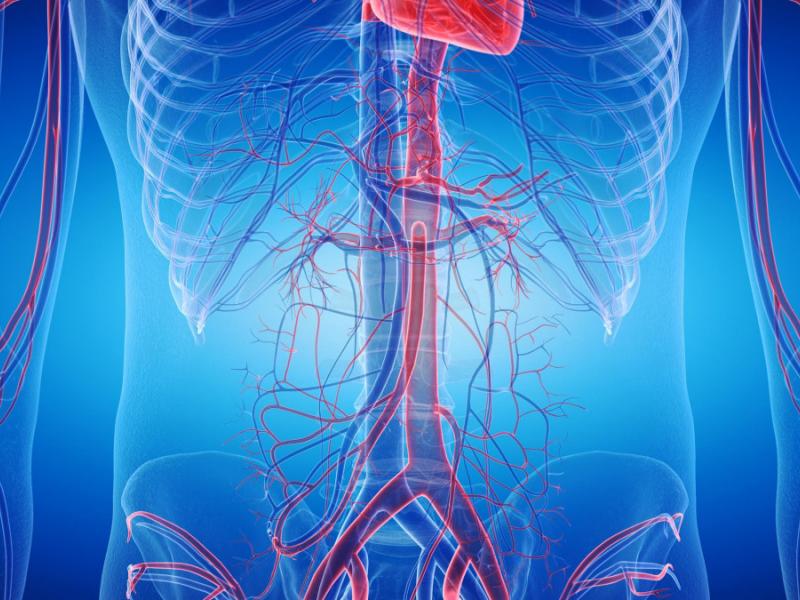

The abdominal aorta does one job, and it does it constantly. It carries oxygenated blood from the heart down through the chest into the abdomen. Every beat, every second. When the wall of this artery starts to weaken, it begins to bulge. That bulge is what doctors call an abdominal aortic aneurysm.
The problem is not the bulge itself. It is what happens when the wall gets too thin. At that point, the artery can rupture, and internal bleeding follows quickly. The window for intervention becomes very small, very fast.
That said, this is not a hopeless diagnosis. Most aneurysms are discovered before they rupture. And when caught early, they can be monitored, managed, and treated effectively.
What Causes an Abdominal Aortic Aneurysm?
There is rarely a single cause. What usually happens is that several factors combine over years to weaken the aortic wall.
Smoking is the one factor that comes up in almost every case. It does not just affect the lungs. The compounds in tobacco work their way into the arterial wall itself, breaking down the connective tissue that keeps the aorta tight and elastic. Years of smoking leave a wall that is thinner, weaker, and far less capable of handling pressure.
High blood pressure tells a different story. There is no visible damage, no dramatic event. Just a constant, invisible force pushing against the vessel wall, every single day. Over time, that pressure wins. The wall stretches. It thins out. It loses the ability to hold its shape.
Atherosclerosis is slower still. Fatty deposits build up gradually on the inside of the arteries, making them stiffer and more brittle. A rigid artery cannot absorb the normal pressure of blood flow the way a healthy one can. Something eventually has to give.
Then there is age. After 65, the risk climbs noticeably, and it climbs faster in men than in women. Nobody fully understands why the gap exists, but the data is consistent. And if a close family member has had an aortic aneurysm, that personal risk goes up again, regardless of lifestyle.
Finally, connective tissue disorders such as Marfan syndrome can trigger aneurysm formation even in younger patients, because the structural proteins that hold the arterial wall together are already compromised from birth.
None of these factors work in isolation. In most patients, it is a combination of two or three of them, building on each other over decades, that finally pushes the arterial wall past its limit.
How Is an Abdominal Aortic Aneurysm Diagnosed?
Here is the uncomfortable truth about abdominal aortic aneurysms: most people who have one do not know it. There are no warning signs in the early stages. No pain, no discomfort, nothing that would send someone to a doctor specifically for this. The aneurysm grows quietly, and it is often picked up by accident, during an ultrasound or CT scan ordered for something else entirely.
That is actually how the majority of cases are found.
When imaging is done specifically to look at the aorta, doctors can measure the diameter of the vessel and spot any abnormal widening. That measurement drives everything that comes next.
Under 5 cm, the aneurysm is considered small. It does not require surgery at that stage, but it does require attention. Regular imaging, typically every 6 to 12 months, is scheduled to track whether it is growing and at what pace.
At 5 cm or above, the risk profile changes. The chance of rupture rises sharply, and most vascular surgeons will start discussing intervention at that point.
Before any treatment decision is made, a full preoperative workup is carried out. This looks at the precise size and position of the aneurysm, checks heart and lung function, and screens for any other aneurysms that may have formed in the legs or elsewhere.
What should not be ignored. Sudden, severe pain in the abdomen or the back is not a normal symptom. In a patient with a known aneurysm, it can mean the wall is about to give way or already has. A pulsating mass felt in the abdomen is another red flag. Neither of these is a wait-and-see situation. Both require emergency care immediately.
Treatment Options for Abdominal Aortic Aneurysm
Treatment is never one-size-fits-all. The size of the aneurysm, how fast it is growing, the patient's overall health, the anatomy of the vessel, all of it goes into the decision. A vascular surgeon will look at the full picture before recommending anything.
Monitoring and Medical Management
For small, stable aneurysms, the first step is usually not surgery. It is structure. Regular imaging keeps a close eye on any changes in size. Blood pressure is controlled carefully. Smoking stops completely. Diet shifts toward reducing cholesterol. Physical activity becomes part of the routine.
This is not passive waiting. It is an active strategy designed to slow the aneurysm down and reduce rupture risk without putting the patient through an operation they do not yet need.
Open Surgical Repair
Once the aneurysm reaches 5 cm or more, the balance tips. The risk of leaving it alone starts to outweigh the risk of operating. Open surgery means going directly into the abdomen, removing the damaged section of the aorta, and replacing it with a synthetic graft, a tube-shaped prosthesis that takes over the job of the weakened vessel.
If the damage has spread into the iliac arteries, the graft is extended to cover those too.
This is a major operation. General anesthesia, several days in the hospital, and a recovery that typically runs four to six weeks. There are real risks, including bleeding, infection, and cardiac stress. But it is also a procedure with decades of proven outcomes behind it, and for complex anatomical cases, it remains the most reliable option available.
Endovascular Repair (EVAR)
EVAR changed the game. Instead of opening the abdomen, the surgeon makes a small incision in the groin and guides a stent graft through the arterial system to the site of the aneurysm. Once it reaches the right position, the graft expands and lines the weakened wall from the inside, cutting the aneurysm off from the circulation.
No large incision. Less blood loss. Lower short-term mortality. Most patients go home within two to three days.
The catch is that not everyone qualifies. The anatomy of the aorta and iliac arteries has to meet specific criteria for EVAR to work safely. And unlike open surgery, it requires long-term imaging follow-up to make sure no blood is leaking back into the aneurysm sac, a complication known as endoleak.
The right choice between EVAR and open repair depends on the individual patient. Age, anatomy, overall health, and surgical risk all factor into that conversation.
Prevention of Abdominal Aortic Aneurysm
Some risk factors are fixed. Age, sex, and family history cannot be changed. But a significant number of aneurysm cases are tied to habits that can be changed.
Stopping smoking is the single most impactful thing a person can do. Keeping blood pressure and cholesterol under control, managing diabetes properly, and staying physically active all reduce the stress placed on the arterial wall over time.
And then there is screening. It is simple, painless, and takes only a few minutes. A one-time abdominal ultrasound is recommended for all men aged 65 and over, particularly those who have ever smoked. It measures the diameter of the aorta and can catch an aneurysm long before it becomes a crisis.
An aneurysm found at 3 cm is a very different situation from one found at 6 cm. That gap is where early detection saves lives.
FAQ: Abdominal Aortic Aneurysm
Can an abdominal aortic aneurysm heal on its own?
No. Once the arterial wall has weakened and dilated, it will not repair itself. Treatment is about preventing growth and rupture, not reversing what has already happened.
Is surgery always necessary?
Not right away. Small aneurysms under 5 cm are usually managed through surveillance and lifestyle changes. Surgery becomes the conversation when the aneurysm hits 5 cm or larger or when it is growing faster than expected.
What happens if an aneurysm ruptures?
It becomes an emergency. Immediately. Survival depends on how fast the patient reaches an operating table. The mortality rate for ruptured aneurysms is high, which is exactly why elective treatment before rupture is so strongly recommended.
Is endovascular repair better than open surgery?
EVAR offers lower short-term risk and a faster recovery. Open surgery is more demanding but can be more durable in certain cases. Neither is universally better. The right choice depends on the patient's anatomy, age, and overall condition.
How long does recovery take?
After EVAR, most patients are back to normal within two to four weeks. After open surgery, expect four to six weeks at minimum, sometimes longer.
Can an abdominal aortic aneurysm be treated in Turkey?
Yes. Vascular surgery in Turkey is performed in JCI-accredited hospitals by experienced specialists at a fraction of the cost compared to Western Europe or North America. A free medical evaluation is available to review your specific case and guide you toward the right option.

"Medical journalist specializing in science communication, I put my expertise at the service of clear and accessible information. For Turquie Santé, I create content based on up-to-date medical data, in collaboration with specialists from partner clinics. My commitment is to provide reliable, transparent information that complies with international medical standards."
Need a personalized medical opinion?
Our partner doctors reply online within 24h, free of charge.