What is Inflammatory Bowel Disease?
Inflammatory bowel disease, or IBD, represents a group of chronic conditions affecting the digestive tract. Unlike occasional digestive upset, IBD involves persistent inflammation of the intestines and colon, characterized by unpredictable cycles. During periods called exacerbations, symptoms flare dramatically. Between these episodes, patients experience remission periods when symptoms subside or disappear entirely.
The underlying cause traces back to an altered immune response. The body's defensive system mistakenly attacks the healthy lining of the gastrointestinal tract, triggering inflammation. Research suggests multiple factors contribute: genetic predisposition, environmental triggers, and dysbiosis (imbalance in gut bacteria). This multifactorial nature means no single cause explains every case.
Two primary forms dominate the IBD spectrum: Crohn's disease and ulcerative colitis. While both share inflammatory characteristics, they differ significantly in location, depth of inflammation, and clinical presentation.
Crohn's Disease: Location and Characteristics
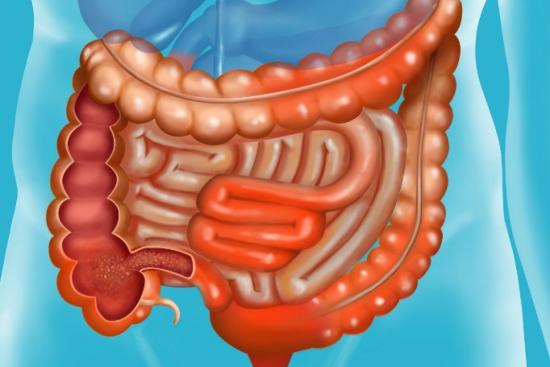
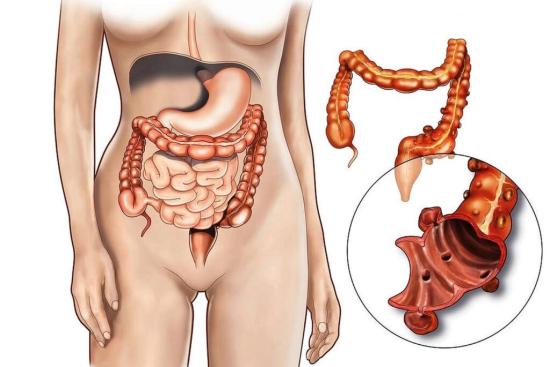
Crohn's disease distinguishes itself by the potential to affect any segment of the digestive tract, from the mouth to the anus. Most commonly, inflammation concentrates in the terminal ileum (the final section of the small intestine) and the colon. However, cases vary. Some patients experience inflammation scattered throughout multiple intestinal regions with healthy segments in between, a pattern called "skip lesions." Others develop complications extending beyond the intestines, affecting the skin, joints, or eyes.
The inflammation in Crohn's disease penetrates deeply into the intestinal wall, reaching all layers. This transmural involvement explains why complications like fistulas (abnormal connections between bowel segments or to the skin), abscesses (pockets of infection), and strictures (narrowed segments) occur more frequently in Crohn's than in ulcerative colitis.
Ulcerative Colitis: Scope and Behavior
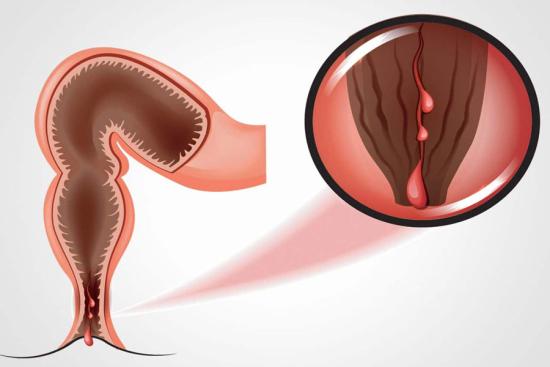
Ulcerative colitis restricts itself exclusively to the colon and rectum. Inflammation affects only the innermost lining of the bowel, not the deeper layers. This distinction matters clinically. While ulcerative colitis generally carries lower complication rates than Crohn's disease, severe flares can necessitate emergency surgery.
The pattern of ulcerative colitis differs too. Inflammation typically begins in the rectum and extends continuously upward into the colon, without skip lesions. Disease extent varies: some patients have inflammation confined to the rectum alone (proctitis), while others experience total colonic involvement.
Diagnosis of Inflammatory Bowel Disease
Accurate diagnosis requires multiple approaches. Colonoscopy remains the gold standard, allowing physicians to visualize the intestinal lining directly and obtain tissue samples (biopsies) for microscopic examination. Biopsies confirm inflammation patterns and rule out infections or malignancy.
For Crohn's disease specifically, additional imaging proves essential. MRI of the abdomen provides detailed visualization of inflammation extending into the small intestine and can detect complications like fistulas or strictures. Ultrasound of the intestinal tract offers real-time assessment and proves particularly useful in pregnant patients, as it avoids radiation exposure.
When Crohn's involves the small intestine, standard colonoscopy cannot reach these regions. Video capsule enteroscopy becomes invaluable, allowing examination of the entire small bowel via a swallowable capsule containing a tiny camera.
Early diagnosis significantly improves outcomes. Prompt identification of IBD allows clinics and hospitals to initiate treatment before complications develop, substantially increasing the likelihood of achieving sustained remission with pharmacological therapies alone.
Symptoms of Crohn's Disease
Symptoms in Crohn's disease vary dramatically depending on which intestinal segment suffers inflammation. Abdominal pain is nearly universal, ranging from mild cramping to severe, debilitating discomfort concentrated around the lower right abdomen. Diarrhea frequently accompanies the pain, sometimes reaching 10-20 episodes daily during severe flares.
Blood in stool occurs but less consistently than in ulcerative colitis. Weight loss develops gradually, reflecting both reduced food intake (due to discomfort and fear of triggering symptoms) and malabsorption of nutrients through damaged intestinal walls. Fatigue often accompanies weight loss, stemming from anemia due to iron deficiency or chronic disease itself.
Systemic manifestations extend beyond the bowel. Joint pain and swelling affect up to 20% of patients. Oral ulcers, eye inflammation (uveitis), and skin lesions (erythema nodosum) occur in a subset of cases. These extraintestinal manifestations sometimes precede gastrointestinal symptoms, complicating early diagnosis.
Symptoms of Ulcerative Colitis
Ulcerative colitis typically presents with bloody diarrhea, often the most distressing symptom. Blood and mucus appear mixed with stool, distinguishing it from simple loose bowel movements. Abdominal cramping accompanies defecation, with frequency potentially reaching 15-20 times daily during severe flares.
Tenesmus, a persistent sensation of incomplete evacuation, drives patients to the toilet despite having just defecated. Urgency feels overwhelming and uncontrollable. Nighttime diarrhea disrupts sleep, amplifying fatigue. Unlike Crohn's disease, weight loss in ulcerative colitis develops primarily from increased diarrhea and reduced oral intake rather than from malabsorption.
Modern Treatment Approaches
Treatment strategies aim for two goals: inducing remission during acute flares and maintaining remission during quiet periods. The arsenal includes several medication classes. 5-aminosalicylates (5-ASAs) provide mild to moderate anti-inflammatory effects, suitable for mild cases or maintenance therapy. Corticosteroids rapidly suppress severe inflammation but carry long-term side effects, limiting their use to acute flares.
Immunosuppressants like azathioprine or 6-mercaptopurine prevent the immune system from attacking the intestine, effective for steroid-dependent patients. Biologic therapies, including TNF-alpha inhibitors and integrin antagonists, represent major advances. These medications target specific immune pathways, achieving remission in patients unresponsive to conventional therapy.
Dietary modifications support medical treatment. Low-residue diets reduce stool volume during acute phases. Certain patients benefit from elimination of specific triggers, though triggers vary individually. Supplements address common deficiencies: iron, vitamin B12, vitamin D, and calcium require monitoring.
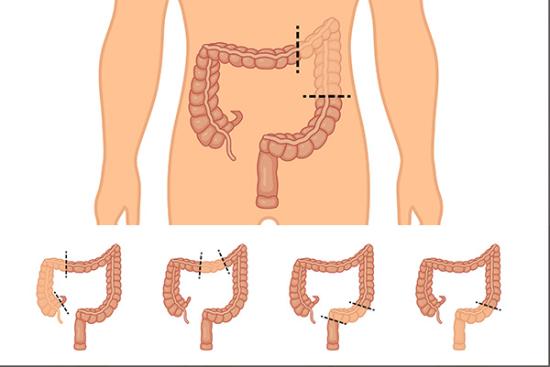
Surgery becomes necessary when medical therapy fails or complications develop. In ulcerative colitis, total colectomy cures the disease but necessitates permanent ileostomy creation or a pouch procedure. In Crohn's disease, surgery typically addresses specific complications rather than curing the disease, as inflammation frequently recurs elsewhere along the digestive tract.
Living with Inflammatory Bowel Disease
IBD profoundly impacts daily life beyond physical symptoms. Unpredictable flares affect work attendance, social activities, and relationships. Anxiety about accessing bathrooms influences travel and public engagement. Many patients experience depression secondary to chronic illness and social isolation.
Effective disease management requires partnership between patient and healthcare team. Regular monitoring through clinical assessment and endoscopic surveillance detects complications early. Stress reduction, adequate sleep, and avoiding known triggers help minimize flare frequency.
For patients seeking specialized gastroenterologic care, colorectal surgery specialists and gastroenterologists at partner clinics can provide comprehensive evaluation and management tailored to individual disease presentation and response patterns.

"Medical journalist specializing in science communication, I put my expertise at the service of clear and accessible information. For Turquie Santé, I create content based on up-to-date medical data, in collaboration with specialists from partner clinics. My commitment is to provide reliable, transparent information that complies with international medical standards."
Need a personalized medical opinion?
Our partner doctors reply online within 24h, free of charge.