If you've been told you need thyroid surgery, you're probably navigating a wave of questions, and understandably so. Is the operation truly necessary? What does it involve exactly? Will I need to take medication for the rest of my life? In medical practice, these concerns come up in virtually every pre-operative consultation, and they deserve clear, honest answers.
Thyroidectomy, the surgical removal of all or part of the thyroid gland, is one of the most frequently performed endocrine surgeries worldwide. The clinics partnered with Turquie Santé have become known for combining internationally accredited surgical expertise with costs that are often 40 to 60% lower than Western European or North American facilities, without compromising clinical standards or safety protocols.
Understanding the Thyroid: Anatomy and Function
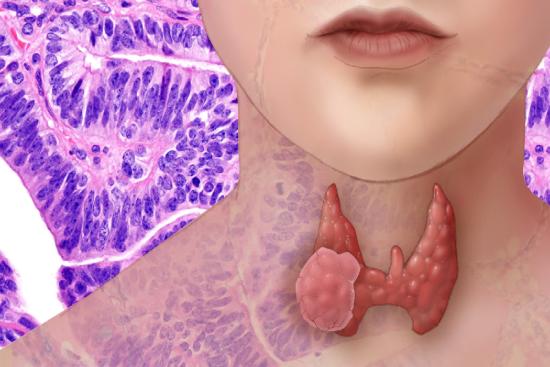
The thyroid is a small, butterfly-shaped gland located at the base of the neck, just below the larynx. Despite its modest size, it plays a central role in regulating your entire metabolism. From heart rate and body temperature to energy levels and weight management, nearly every cell in your body depends on thyroid hormones. The gland produces two key hormones: thyroxine (T4) and triiodothyronine (T3).
When functioning properly, thyroid hormones maintain a delicate balance. Too much or too little disrupts this equilibrium. T4 and T3 regulate how quickly your cells burn calories, how fast your heart beats, and even how efficiently your nervous system responds to stimuli. This is why thyroid dysfunction can feel so widespread, fatigue, weight changes, mood swings, or heat intolerance often have their root cause in this small gland.
When Is Thyroidectomy Recommended?
Several conditions warrant surgical intervention. Thyroid cancer, whether papillary, follicular, or medullary, almost always requires removal of all or part of the gland. The extent depends on tumor type, size, and whether lymph nodes are involved.
Hyperthyroidism that doesn't respond to medication or radioactive iodine is another common indication. Graves' disease, toxic nodules, or toxic multinodular goiter can overload your system with hormones, causing palpitations, tremor, anxiety, and weight loss. Surgery offers definitive relief when other treatments fail.
Large goiters, whether benign or partially toxic, can cause physical compression. Patients report difficulty swallowing, breathing problems, or a sensation of choking. Some describe the gland pressing against the windpipe during sleep. In cases where structural breathing issues are present, surgeons must assess airway integrity thoroughly.
Nodules with uncertain diagnosis (indeterminate cytology on fine-needle biopsy) sometimes require hemithyroidectomy (removal of one lobe) for definitive histological examination. Not all nodules need removal, many remain stable for years, but when suspicion is high or growth is documented, surgery eliminates uncertainty.
Thyroiditis (inflammation) or autoimmune conditions occasionally warrant surgery if complications arise, though this is less common. Your endocrinologist and surgeon will evaluate imaging, blood work, and symptoms to determine if your specific situation calls for thyroidectomy.
Types of Thyroidectomy Surgery
Surgeons don't always remove the entire gland. The approach depends entirely on your diagnosis and risk profile.
Total thyroidectomy removes the entire gland. This is standard for thyroid cancer, as any remaining tissue could harbor malignant cells. It's also chosen for diffuse hyperthyroidism (Graves' disease) to prevent recurrence. After total removal, lifelong levothyroxine replacement becomes necessary.
Hemithyroidectomy (or partial thyroidectomy) removes only one lobe, preserving the other. This approach works when cancer is confined to one side, nodules are unilateral, or when preserving some thyroid function is desirable. The remaining lobe often compensates adequately, though some patients eventually need supplemental hormone therapy.
Subtotal thyroidectomy leaves a small amount of thyroid tissue (usually 2-4 grams) on one or both sides. This technique, less common today, aims to preserve some hormone production while removing the bulk of diseased tissue. It carries a risk of recurrent hyperthyroidism if the remnant tissue remains overactive.
The surgeon's choice reflects a balance: removing enough diseased tissue to treat your condition while preserving function where possible. Imaging studies (ultrasound, CT, or MRI) and thyroid function tests guide this decision beforehand.
Preparation and Preoperative Assessment
Before surgery, several evaluations occur. Blood tests measure TSH, free T4, and free T3 to establish baseline function. If you have hyperthyroidism, your surgeon may prescribe beta-blockers (propranolol) or antithyroid drugs (methimazole, PTU) to bring hormone levels under control, operating on a severely hyperthyroid patient risks thyroid storm, a life-threatening complication.
Imaging is crucial. Thyroid ultrasound identifies nodule location, size, and characteristics. If thyroid cancer is suspected, ultrasound guides whether additional imaging (CT, MRI) or staging scans are needed. Some surgeons request laryngoscopy to assess vocal cord function beforehand, especially if there's concern about recurrent laryngeal nerve involvement from a large mass.
Your anesthesiologist will review your medical history, current medications, and allergies. If you take blood thinners, you'll typically pause them days before surgery. Some supplements (especially iodine-containing ones) should be stopped temporarily. Bring a complete medication list to your preoperative consultation.
At the partnered clinics in Turkey, pre-operative workup is thorough. Patients often arrive a day or two early to complete final labs and imaging, reducing uncertainty on surgery day. This organized approach is standard across accredited Turkish surgical centers.
The Surgical Procedure: What Happens in the Operating Room
Thyroidectomy typically lasts 1 to 2 hours, though complex cases may take longer. You'll be under general anesthesia with endotracheal intubation (a breathing tube). The surgeon makes an incision in the neck, usually a 3- to 5-centimeter horizontal line just below the larynx, often in a natural skin crease. Some surgeons now use minimally invasive techniques with smaller incisions or even robot-assisted approaches, though traditional open surgery remains the standard.
Once the incision is open, the surgeon identifies the thyroid gland and its surrounding structures. Two critical nerves demand meticulous care: the recurrent laryngeal nerves (which control vocal cord movement) and the superior laryngeal nerves (which control voice pitch). Injury to these causes hoarseness or voice weakness. Modern surgical technique often includes intraoperative nerve monitoring, small electrodes detect nerve activity, alerting the surgeon if manipulation is threatening function.
The parathyroid glands, four tiny structures embedded in or near the thyroid, are identified and preserved. They regulate calcium and phosphate metabolism. Accidentally removing or devascularizing them causes hypoparathyroidism, with symptoms like numbness, muscle cramps, or tetany from low blood calcium.
Depending on your diagnosis, the surgeon removes one lobe, both lobes, or both with the central lymph nodes (if cancer is present). Bleeding vessels are sealed with ties, clips, or cautery. The incision is closed in layers, typically with absorbable stitches under the skin and clips or staples on the skin surface. These are removed 5 to 7 days later.
Potential Complications and Recovery
Thyroidectomy is generally safe, but like any surgery, risks exist. Most patients experience mild neck discomfort and soreness for a few days. Pain is usually manageable with acetaminophen or mild opioids for the first 24 to 48 hours.
Hoarseness or voice changes occur in roughly 1 to 2% of patients when the recurrent laryngeal nerve is injured. Usually this improves within weeks to months as the nerve recovers or the body adapts. Permanent hoarseness is rare with experienced surgeons.
Hypoparathyroidism (low parathyroid function) causes low blood calcium. Symptoms include tingling lips, fingers, and toes, muscle cramps, or in severe cases, seizures. This happens in about 1 to 3% of cases. Many resolve spontaneously within days or weeks as parathyroid blood flow restores. Temporary supplementation with calcium and vitamin D may be needed.
Bleeding or hematoma (blood collection) is rare but requires monitoring. A small amount of blood in the surgical site is normal, but significant bleeding can compress the airway, watch for increased neck swelling, difficulty breathing, or difficulty swallowing immediately after surgery.
Infection is uncommon with prophylactic antibiotics. If fever, increasing redness, or drainage develops in the following days, contact your surgeon promptly.
Most patients go home the same day or after one overnight stay. Walking and light activity resume within a few days. Heavy lifting and strenuous exercise wait 2 to 3 weeks to allow the incision to heal fully.
Postoperative Hormone Management
If your entire thyroid was removed, you'll take levothyroxine (synthetic T4) for life. Dosing starts at a standard amount (often 50 to 75 micrograms daily) and is adjusted based on TSH levels checked 6 to 8 weeks after surgery. The goal is to keep TSH in a target range, usually 0.5 to 2.5 mIU/L for most patients, though cancer survivors may need suppressed TSH levels to prevent recurrence.
If one lobe remains, thyroid function often stabilizes without supplementation. However, gradual thyroid failure can develop over months or years, so periodic TSH testing is prudent.
Levothyroxine should be taken on an empty stomach, 30 to 60 minutes before breakfast, for optimal absorption. Calcium, iron, and certain other supplements interfere with absorption, so spacing them out matters.
Some patients need combination therapy with T4 and T3 (liothyronine) if symptoms of hypothyroidism persist on T4 alone, though this is debated among endocrinologists. Discuss your symptoms and lab results with your doctor, medication adjustment often resolves fatigue or weight gain.
Why Choose Turkey for Thyroidectomy?
Turkish surgical centers have earned international accreditation (JCI, ISO) and employ surgeons trained in Europe, North America, and Turkey itself. The clinics partnered with Turquie Santé offer state-of-the-art operating rooms, intraoperative monitoring, and postoperative care comparable to Western hospitals.
Cost is a significant advantage. A thyroidectomy in Turkey typically costs 30 to 50% of the equivalent procedure in the US or Western Europe. This affordability doesn't reflect lower standards, rather, it reflects lower overhead and healthcare system economics. Many patients combine surgery with a brief recovery holiday, making the trip worthwhile financially and personally.
The patient experience is often smoother abroad. Dedicated coordinators handle logistics, arrange preoperative consultations, schedule imaging, and organize accommodation. Language support is standard. Recovery packages sometimes include hotel stays, airport transfers, and follow-up telemedicine appointments with your surgeon after you return home.
That said, choosing a surgeon matters more than geography. Comprehensive pre-operative checkups and consultations with your medical team ensure clarity before committing to any surgical destination. Ask about surgeon experience, complication rates, and patient testimonials. Turquie Santé connects you with verified clinics, but your due diligence is essential.
Recovery Timeline and Return to Normal Activities
Week one post-surgery is the most restricted. Avoid heavy lifting, driving (if pain or pain medication limits you), and strenuous activity. Walking is encouraged. Neck mobility improves as swelling subsides. Most patients report feeling significantly better by day 5 to 7.
By week two, light office work and daily activities resume for many. The incision becomes less tender. Some redness or slight drainage may persist, this is normal as long as there's no sign of infection (fever, increasing redness, foul odor).
Week three onward, exercise can resume gradually. Start with light cardio (walking, swimming) and progress to weight training only after your surgeon clears you, usually 3 to 4 weeks post-op.
Scar maturation takes months. Initially red and raised, the scar gradually flattens and fades. Silicone scar sheets or massage (after the incision is fully closed) may improve appearance. Most scars become nearly invisible within 6 to 12 months, especially if hidden by the neck or a collar.
Alternative Treatments to Consider
Not every thyroid condition requires surgery. Hyperthyroidism can sometimes be managed with antithyroid drugs (methimazole, PTU) or radioactive iodine ablation. When diagnosis is uncertain, biopsy guidance techniques help clarify whether nodules are benign or malignant, sometimes avoiding unnecessary surgery.
Benign nodules detected incidentally often need only monitoring with periodic ultrasound, many never grow or cause symptoms. Radioactive iodine works well for hyperthyroidism in some patients, though it inevitably causes permanent hypothyroidism requiring lifelong levothyroxine.
The choice between surgery, medication, and radioactive iodine depends on your diagnosis, age, and preferences. Your endocrinologist and surgeon will discuss trade-offs. Surgery offers definitive treatment for cancer and large goiters, while medication buys time or avoids surgery in some cases.
Questions to Ask Your Surgeon Before Surgery
Prepare a list for your preoperative consultation. Ask about the planned extent of surgery (total vs. partial). Inquire about nerve monitoring and how it's performed. Ask the surgeon's complication rate for recurrent laryngeal nerve injury and hypoparathyroidism. How many thyroidectomies does he or she perform annually? What's the typical hospital stay? When can you resume normal activities and exercise? Who monitors you after you return home, can you reach the surgical team if complications arise? Understanding these details reduces anxiety and sets realistic expectations.
If traveling to Turkey, ask about postoperative support. Can you have follow-up appointments by video call? If complications occur after you return home, who coordinates with your local doctor? Reputable clinics partnered with Turquie Santé offer telemedicine follow-up, removing the burden of traveling back for routine checks.
Life After Thyroidectomy
Most patients return to fully normal life within weeks. The main ongoing commitment is taking thyroid hormone replacement (if applicable) consistently and having TSH levels checked annually. Many report improved energy, mood, and well-being once hormone levels stabilize postoperatively.
If you had cancer, you may need periodic surveillance scans (ultrasound, radioactive iodine scan, or CT) to monitor for recurrence, depending on cancer stage. Your oncologist will outline this plan.
Pregnancy is possible after thyroidectomy. Women should ensure TSH is well-controlled before conception, as thyroid hormone needs often increase during pregnancy. Coordination between your obstetrician and endocrinologist ensures safe dosing.
The incision scar eventually becomes a thin line, often barely visible. Many patients find their only lasting reminder is the need for daily levothyroxine, a small price for definitive treatment of a serious thyroid condition.

"Medical journalist specializing in science communication, I put my expertise at the service of clear and accessible information. For Turquie Santé, I create content based on up-to-date medical data, in collaboration with specialists from partner clinics. My commitment is to provide reliable, transparent information that complies with international medical standards."
Need a personalized medical opinion?
Our partner doctors reply online within 24h, free of charge.