Millions worldwide struggle with vision problems that shape how they experience daily life. Reading becomes tedious, driving after sunset grows risky, and screens blur into an unsolvable problem. Fortunately, modern ophthalmology has transformed. The convergence of laser precision and advanced surgical implants now offers real solutions where glasses and contact lenses once seemed the only path.
Two procedures stand out in this landscape: intraocular lens (IOL) implantation and Presbyond laser treatment. Both reshape how light enters and focuses on the retina, yet they work through fundamentally different mechanisms. Understanding their differences matters because the right choice depends on your specific eye anatomy, lifestyle, and long-term vision goals.
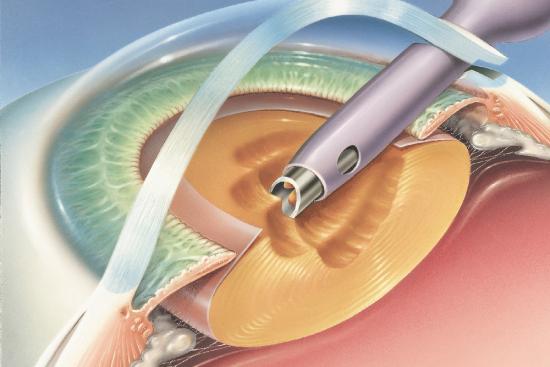
Understanding Intraocular Lens Implantation
IOL implantation represents a surgical shift from correction to replacement. Rather than reshaping the cornea with a laser beam, this procedure removes your eye's natural lens and substitutes it with a precision-manufactured artificial one.
The surgery typically addresses cataracts, but modern implant technology has expanded its applications. Intraocular lens implants now treat presbyopia, myopia, hyperopia, and astigmatism in patients who may not be candidates for laser procedures. The artificial lens remains permanently in place, requiring no maintenance or replacement in most cases.
What makes IOL compelling: the procedure works regardless of corneal thickness. Patients with thin corneas, irregular astigmatism, or previous refractive surgery often find IOL their best option. The results tend to be stable, with minimal regression over decades. Multifocal IOLs even address presbyopia directly, allowing simultaneous focus at multiple distances. Some patients report sharper contrast sensitivity compared to preoperative vision, particularly in low-light environments.
Recovery unfolds gradually. Most regain functional vision within days, though optimal results emerge over 4 to 6 weeks as corneal swelling subsides and neural adaptation occurs. You can resume light activities almost immediately, though strenuous exercise typically waits 3 to 4 weeks.
Limitations exist. IOL is an invasive surgical procedure with inherent risks, including infection, inflammation, or posterior capsular opacification (a clouding that may require a minor follow-up laser treatment). Presbyopia symptoms may persist even with multifocal lenses, and some patients experience halos or glare, especially at night. Cost considerations apply, particularly for premium IOL designs.
The Presbyond Laser Approach
Presbyond laser technology reshapes the cornea itself rather than replacing internal structures. Using excimer laser pulses, the procedure sculpts the corneal surface to create a multifocal pattern, allowing simultaneous focus at near and distance.
The attraction is straightforward: non-surgical simplicity and rapid results. The procedure takes minutes. You walk in, spend 15 to 20 minutes under the laser, and leave with clearer vision within hours. Most patients achieve 90 percent of final results by day three, and full stabilization occurs within 2 to 3 months.
Presbyond works particularly well for patients aged 40 to 55 experiencing early presbyopia alongside myopia or hyperopia. The monovision correction principle underlies the treatment: one eye prioritizes distance vision while the other favors near tasks. Your brain adapts to this asymmetry within weeks. Some patients report excellent intermediate vision without the optical trade-offs of traditional monovision contact lenses.
Not all candidates qualify. Corneal thickness matters critically. The laser ablates (removes) a specific corneal layer, and insufficient remaining tissue (stromal bed) after treatment creates instability. Patients with thin corneas often cannot proceed. Irregular astigmatism, keratoconus suspects, or previous refractive surgery sometimes contraindicate the procedure. Additionally, Presbyond femtosecond treatment produces reversible results in principle but practical reversal through re-treatment carries cumulative risk.
Dry eye symptoms emerge frequently in the immediate postoperative weeks. While typically mild and manageable with drops, some patients experience persistent dryness months later. Glare and halos occur, usually diminishing over time but occasionally lingering. Reversibility is theoretically possible through additional laser work, but it demands caution and adds cost.
Comparing Key Surgical Factors
Invasiveness: IOL surgery involves anesthesia and a corneal or scleral incision, making it genuinely invasive. Recovery includes infection and inflammation risks inherent to any surgery. Presbyond uses no blade and causes no structural incision, only corneal sculpting. Recovery is faster and infection risk minimal.
Candidacy scope: IOL suits nearly anyone, including thin-cornea patients, those with extreme refractive errors, and post-LASIK eyes. Presbyond remains limited by corneal thickness and stability. Irregular astigmatism often disqualifies candidates.
Visual outcomes: Both achieve similar uncorrected visual acuity for most patients, typically 20/20 or better for distance. IOL generally offers superior contrast in low light. Presbyond multifocal patterns sometimes produce edge glare that IOL avoids. Intermediate vision varies by patient and technology generation.
Longevity: IOL lasts indefinitely in nearly all cases, though technology evolution means future upgrades remain possible through lens exchange. Presbyond results remain stable, though some regression occurs (typically less than 10 percent) over 5 to 10 years.
Cost structure: IOL typically ranges higher upfront but spreads across decades. Presbyond appears cheaper initially but additional treatments may accumulate costs. Consider insurance coverage, which sometimes differs between procedures.
Dry Eye and Comfort Considerations
Postoperative comfort diverges significantly. IOL surgery temporarily disrupts the ocular surface but heals completely in weeks. Dry eye usually resolves as the cornea stabilizes. Presbyond induces more consistent dry eye through its corneal remodeling mechanism. Some studies suggest 20 to 40 percent of patients experience moderate dryness lasting months. Pre-existing dry eye predicts worse outcomes with Presbyond, making pre-treatment screening essential.
Intensive lubrication protocols help both procedures, but Presbyond may demand longer supplementation. Punctal plugs (tiny inserts that reduce tear drainage) sometimes justify placement before Presbyond. IOL patients rarely need such measures.
Night Vision and Optical Quality
Presbyond's multifocal corneal pattern creates optical compromises. Light distribution across multiple focal points reduces contrast in dim environments. Some patients report halos around streetlights or car headlights, particularly in the first months. Most experience resolution as neural adaptation reorders the visual signal. IOL multifocals also create halos, but the optical quality tends sharper because the lens sits behind the pupil, benefiting from pupillary diffraction patterns.
Distance acuity sharpness favors IOL in careful comparison studies, though the difference remains clinically modest for most patients. Presbyond excels when intermediate vision (computer screens, dashboard displays) matters equally.
Recovery Timeline and Activity Restrictions
Presbyond accelerates return to function dramatically. Most resume normal activities within 48 hours. Swimming, contact sports, and manual labor can restart after one week once epithelial healing completes. Full visual stability takes 3 months, but meaningful improvement arrives within days.
IOL recovery proceeds more cautiously. Physical activity restrictions typically span 3 to 4 weeks. Swimming and hot tubs must wait 2 weeks minimum due to infection risk. Full visual stability emerges over 4 to 6 weeks. This longer timeline reflects the surgical nature of the intervention.
Professional athletes sometimes favor Presbyond for its rapid return timeline, though IOL remains an option if scheduled during off-season. The specific sport matters. Contact sports post-IOL demand protective eyewear even after healing because the artificial lens lacks the eye's natural protective response to trauma.
Retreatment Options and Reversibility
Presbyond retreatment remains possible if over-correction or under-correction occurs. Additional laser applications can fine-tune results, though repeated ablation accumulates corneal thinning. Generally, one enhancement laser session poses minimal risk, but two or three compounds concerns. The procedure fundamentally cannot fully reverse; once corneal tissue ablates, restoration requires corneal graft surgery (rarely performed for refractive reasons).
IOL exchange is feasible if power miscalculation or changing refractive error demands adjustment. Surgeons can swap the implant relatively safely, though the procedure carries identical risks as the original surgery. Refractive surprise (unexpected postoperative refractive error) occurs in perhaps 10 to 15 percent of cases, making post-operative fine-tuning via wavefront laser (LASIK enhancement) sometimes necessary.
Special Populations and Age Considerations
Patient age subtly reshapes decision-making. Presbyond optimally suits patients aged 40 to 60 where presbyopia represents the primary concern. Younger patients with simple myopia or hyperopia may prefer standard LASIK or PRK rather than presbyopia-targeting Presbyond. Older patients (65+) sometimes benefit more from IOL because presbyopia becomes less relevant when spectacle needs for reading remain likely anyway.
Post-LASIK patients pose a specific challenge. Previous corneal surgery reduces corneal thickness and distorts the optical surface. IOL bypasses these concerns entirely, making it often superior for this population. Presbyond becomes riskier due to pre-existing thinning.
Patients with severe astigmatism (3.0+ diopters) generally achieve better outcomes with IOL because toric implants address the astigmatic component through internal optics rather than corneal sculpting. Presbyond multifocal patterns struggle with simultaneous cylindrical correction.
Questions to Discuss with Your Ophthalmologist
Before committing, clarify specific parameters. Ask for measured corneal thickness and wavefront analysis results. Determine whether your particular refractive error favors one procedure over the other. Discuss realistic postoperative visual expectations, including likelihood of spectacle dependence for specific tasks. Inquire about dry eye risk factors specific to your ocular surface. Request information about your surgeon's personal complication rates for each procedure, not just literature averages. Finally, understand revision procedures, their costs, and their likelihood in your case.
The clinics partnered with Turquie Santé maintain expertise in both techniques and can guide you toward the most suitable approach based on detailed preoperative assessment. Advanced imaging now permits precise candidacy determination, eliminating guesswork.

"As I am passionate about science, I studied optometry which I eventually gave up. In the midst of it all, I fell in love with the editorial staff.I think that the best form of generosity is to share your knowledge after consulting a number of encyclopedias. "
Need a personalized medical opinion?
Our partner doctors reply online within 24h, free of charge.