


The deep plane facelift has accumulated significant marketing capital over the past decade. The question worth asking is: Does the clinical evidence justify the premium?
Two systematic reviews published in 2025 now provide the clearest answer to date. A meta-analysis in Aesthetic Plastic Surgery analysing 2,896 patients found deep plane satisfaction at 94.4% versus 87.8% for SMAS, a statistically significant difference. A second review in the Annals of Plastic Surgery, covering 10,766 patients across 47 studies, identified midface restoration as the domain of unambiguous deep plane superiority.
This article analyses the practical implications of those findings, including the complications data that advocates rarely highlight, and maps the evidence onto the clinical decision of which technique is appropriate for which patient.
The anatomical rationale: Why going bigger changes everything
Facial ageing is not primarily a skin problem. The visible signs, jowls, nasolabial folds, and malar flattening result from the progressive inferior displacement of deep anatomical structures: retaining ligaments, deep fat compartments, and the SMAS itself. Addressing only the skin treats the downstream effect, not the upstream cause.
What the Deep Plane does that SMAS cannot:
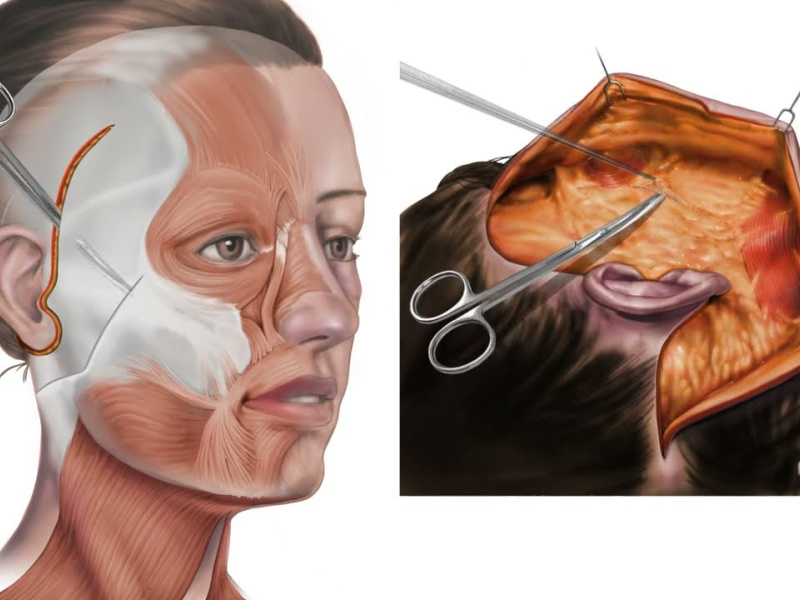
- Retaining ligament release: the zygomatic and masseteric ligaments, the primary anchors tethering facial soft tissue to bone, are released, permitting true repositioning rather than mere suspension.
- En bloc tissue elevation: skin, SMAS, and deep fat are elevated as a single composite unit along the natural rejuvenation vector (superoposterior), eliminating the mechanical tension on skin that produces the operated appearance.
- Direct midface access: malar fat compartments and nasolabial tissue, structurally inaccessible to SMAS dissection, are mobilised and repositioned directly.
- Expression preservation: because facial animation musculature is not placed under tension, normal dynamic expression is maintained, a critical distinction for long-term naturalness.
Evidence-based comparison: Deep Plane vs SMAS
The following table synthesises the 2025 meta-analyses alongside established clinical data:
| Criterion | Deep Plane | SMAS Facelift |
| Dissection level | Sub-SMAS - releases retaining ligaments + deep fat compartments | SMAS layer only - no ligament release |
| Mechanism | Elevates skin, SMAS, and deep fat as a single anatomical unit | Implicates or plications the SMAS without liberating deep attachments |
| Midface restoration | Excellent - malar fat, nasolabial folds directly addressed | Limited - historically the SMAS Achilles' heel |
| Result naturalness | Very natural - face mobilises normally with expression | Good, but excess skin tension can create a pulled appearance |
| Result longevity | 10–15 years | 7–10 years |
| Patient satisfaction (2025) | 94.4% (PubMed meta-analysis, 2,896 patients) | 87.8% (same meta-analysis) |
| Complication rate | 17.2% | 10.3% |
| Recovery | 3–4 weeks | 2–3 weeks |
| Surgeon requirement | Advanced specialist training - steep learning curve | Experienced plastic surgeon |
Where the evidence is strongest, and where is it not?
Deep plane facelift offers clear anatomical advantages, but the evidence isn’t uniform across all areas. Here’s where it excels—and where caution is warranted.
Midface: the most consistently proven advantage
The meta-analysis by Vayalapra et al. (2025), including 10,766 patients, demonstrates a clear and reproducible benefit of deep plane facelifts in the midface. By lifting the malar fat pads, correcting nasolabial folds, and repositioning the midface as a unit, deep plane addresses the areas where SMAS-only procedures historically underperform. SMAS techniques, designed primarily for the lower face and neck, often leave the midface less fully corrected.
Longevity: structural rationale supported by data
The 10–15 year durability of deep plane results follows logically from its mechanism. By releasing and repositioning ligaments and deep tissue as a cohesive unit, the procedure reduces the recurrence of ptosis that occurs when only the skin or superficial SMAS is tightened. Longitudinal follow-up studies consistently show deep plane outcomes remaining superior at 5–7 years when compared to SMAS cohorts treated in the same period.
Complications: the honest counterargument
Deep plane has a slightly higher complication rate: 17.2% versus 10.3% for SMAS. Most complications are minor (Grade I–II), such as prolonged edema, transient hypoesthesia, or minor hematoma, and typically resolve without intervention. Permanent facial nerve injury, the complication most feared by patients, is very rare, under 1% in experienced hands.
Critical caveat: these statistics derive from high-volume specialist centers. In lower-volume or less experienced settings, complication rates rise. Deep plane is not a technique that safely translates to occasional practitioners without extensive training.
Counterevidence: when SMAS can match the deep plane
Rigorous scientific evaluation requires acknowledging dissenting data. Comparative studies show that highly experienced surgeons performing High SMAS facelifts can achieve outcomes comparable to deep plane results, often with fewer complications. This underscores a critical point: surgeon expertise remains the single most important determinant of outcome, sometimes outweighing the choice of technique.
Clinical indications: Patient selection for Deep Plane
Deep plane facelift is not indicated for every patient. Its benefits are most pronounced in specific anatomical and clinical scenarios:
- Manifest midface ptosis: Significant descent of the malar region, deep nasolabial folds, and jowling represent the primary indication. Deep plane directly addresses these changes at their structural origin.
- Revision after prior SMAS facelift: In patients with previous SMAS surgery and suboptimal or recurrent results, deep plane offers access to untouched anatomical planes. This makes it the preferred option for secondary or revision procedures.
- Dense or heavy facial morphology: thick soft tissue does not respond reliably to SMAS suspension; ligament release and en bloc elevation are typically superior.
- Preventive deep plane (35–45): a 2025 AAFPRS trend, early intervention when tissue quality is optimal, produces longer-lasting, more natural results at lower technical difficulty
- When SMAS remains appropriate: mild laxity, isolated lower face and neck treatment, patients prioritising shorter recovery, practitioners without advanced deep plane training
Technique selection should be driven by anatomy and surgeon expertise, not by trend alone.
Technical evolution in 2026
The deep plane is not static. Three developments will define the clinical landscape in 2026:
- Extended Deep Plane: Dissection is extended to the periorbital region and temporal area for comprehensive, single-session facial rejuvenation, including the upper and midface in one anatomical plane.
- Deep Plane + Structural fat grafting: Simultaneous volume restoration (lipofilling) combined with structural lifting in a single operative session addresses the descent and volumetric loss associated with facial aging.
- Accelerated recovery protocols: Advanced anesthetic techniques and lymphatic drainage protocols have reduced the social recovery period to 10–14 days in leading centers, narrowing the gap with SMAS.
- AI-assisted surgical planning: 3D morphometric analysis and simulation software are increasingly used for preoperative planning and patient communication in specialized centers.

"Medical journalist specializing in science communication, I put my expertise at the service of clear and accessible information. For Turquie Santé, I create content based on up-to-date medical data, in collaboration with specialists from partner clinics. My commitment is to provide reliable, transparent information that complies with international medical standards."