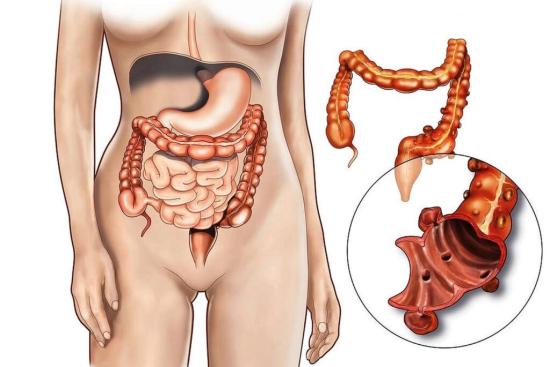
You've been dealing with constipation for months, sometimes years, despite trying fiber, laxatives, and even pelvic floor therapy. When these approaches fail, and symptoms become severe, surgery may become not just an option, but the only effective solution.
This is the question many patients hesitate to ask: “Have I reached the point where surgery is necessary?”
Too often, the answer is delayed, either because of embarrassment or simply because patients are not aware that surgical treatment exists.
For a carefully selected group of patients with chronic, treatment-resistant constipation, surgery can significantly improve quality of life. Today, this option is performed in specialized centers with expertise in digestive surgery, including in countries such as Turkey.
Cost of chronic constipation surgery: Turkey vs. other countries
All prices are approximate and inclusive of surgeon fees, anesthesia, and standard admission.
| Procedure | Turkey ($) | UK (£) | Germany (€) | USA ($) | Notes |
| Full diagnostic workup (manometry + transit study + colonoscopy) | 440–880 | 1,200–2,000 | 1,200–2,000 | 2,000–4,000 | Includes complete preoperative evaluation; Istanbul clinics provide 1–2 day completion without waiting lists |
| Anorectal surgery (rectopexy, rectocele repair, STARR) | 1,650–3,080 | 4,000–7,000 | 4,000–7,500 | 6,000–12,000 | Minimally invasive procedures; hospital stay 1–3 days; excellent functional outcomes when anatomy is well-documented |
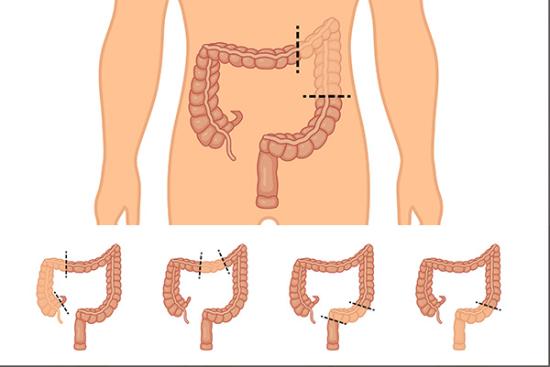
| Laparoscopic subtotal colectomy (ileorectal anastomosis) | 3,300–5,500 | 8,000–14,000 | 8,000–13,000 | 15,000–30,000 | Standardized in expert colorectal centers; hospital stay 4–6 days; post-op nutrition follow-up recommended |
| Sacral neuromodulation (test + permanent implant) | 2,750–4,950 | 6,500–11,000 | 7,000–12,000 | 12,000–25,000 | For selected patients with refractory constipation or incontinence; includes device, implantation, and follow-up |
Sources & notes:
- Turkey prices: Verified with Turquie Santé JCI-accredited partner clinics, inclusive of surgeon fees, anesthesia, and standard admission.
- UK & Germany: Private hospital guide prices.
- USA: CareCredit / Healthline 2024 data.
- Out-of-pocket costs vary; NHS, statutory insurance, or private coverage may reduce patient contribution.